Table of Contents >> Show >> Hide
- Why Getting the Right Rheumatoid Arthritis Diagnosis Matters
- Step One: Your Story and the Physical Exam
- Key Blood Tests in Rheumatoid Arthritis Diagnosis
- Imaging: Seeing Rheumatoid Arthritis in Your Joints
- The 2010 ACR/EULAR Classification Criteria: The Scoring System Behind RA
- Conditions That Can Mimic Rheumatoid Arthritis
- What the RA Diagnostic Journey Often Looks Like
- Living in the “Maybe” Zone: Undifferentiated Arthritis
- How Often Are Tests Repeated?
- Real-Life Experiences with Rheumatoid Arthritis Diagnosis
- The Bottom Line
If your joints have been stiff, swollen, and acting like they’re 90 years old while the rest of you is not, you might have already asked the big question:
“Could this be rheumatoid arthritis?” (And then immediately asked Dr. Google, which is how you probably ended up here.)
Rheumatoid arthritis (RA) is a chronic autoimmune disease that can quietly damage joints and even organs long before it’s officially named.
The good news: modern rheumatoid arthritis diagnosis tools are much better than they used to be, and many people get an answerand a treatment planmuch earlier in the disease course.
In this guide, we’ll walk through how doctors diagnose RA, what tests are typically used, how the official ACR/EULAR criteria work, and what the whole process looks like from a patient’s point of view.
No medical degree requiredjust a willingness to learn a bit about your joints and immune system.
Why Getting the Right Rheumatoid Arthritis Diagnosis Matters
RA isn’t just “normal wear-and-tear arthritis.” It’s an autoimmune condition, meaning your immune system accidentally targets the lining of your joints.
Left unchecked, this inflammation can lead to joint damage, deformity, disability, fatigue, and even heart and lung complications.
The key phrase you’ll hear over and over is “early diagnosis and early treatment.”
Doctors now aim to identify RA as soon as possible so they can start disease-modifying antirheumatic drugs (DMARDs).
These medications don’t just help symptomsthey can slow or prevent further joint damage.
That’s why modern RA diagnosis is not based on one magic test. It’s a puzzle assembled from your symptoms, physical exam, blood work, imaging, and formal classification criteria.
Think of your doctor as a detective, and all of these are clues pointing toward (or away from) RA.
Step One: Your Story and the Physical Exam
Your Medical History: What Your Doctor Will Ask
Before any blood test or X-ray, your doctor will start with a conversation. Be prepared for questions like:
- Which joints hurt? RA often starts in the small joints of the hands, wrists, and feet, and usually affects both sides of the body.
- How long have you had symptoms? RA tends to stick around for more than six weeks, not just a few days.
- What is morning like? Classic RA includes morning stiffness that can last an hour or more and gradually improves with movement.
- Any family history? Autoimmune diseases can run in families, even if relatives have different conditions such as lupus, thyroid disease, or psoriasis.
- Whole-body symptoms? Fatigue, low-grade fevers, weight loss, or feeling generally unwell can support the suspicion of systemic inflammation.
Don’t hold back because you’re afraid of “overreacting.” When it comes to RA, a thorough story is a gift to your rheumatologist.
Physical Exam: What Doctors Look for in Your Joints
During the physical exam, your provider will:
- Check for swelling, warmth, and tenderness in many joints, especially hands, wrists, elbows, knees, ankles, and feet.
- Look for a symmetrical pattern (for example, both wrists or both knees).
- Assess your range of motionhow far you can bend or straighten each joint.
- Watch how you move, grip, or walk to see how joint symptoms affect daily activities.
- Look for signs outside the joints, such as nodules under the skin, eye redness, or rashes that might suggest another autoimmune disease.
If your doctor finds at least one joint with clear inflammatory swelling that doesn’t seem to be explained by an injury or another condition, RA jumps higher on the “suspect list.”
Key Blood Tests in Rheumatoid Arthritis Diagnosis
Here’s a slightly annoying truth: there is no single blood test that proves you have RA or proves that you don’t.
Lab tests are pieces of evidenceuseful, but not the entire verdict.
Rheumatoid Factor (RF)
Rheumatoid factor is an antibody that many people with RA have. A positive RF test can support the diagnosis, especially if levels are high.
However, RF is not exclusive to RA:
- Some people with other autoimmune or chronic infections can test positive.
- Older adults without RA sometimes have a low positive RF.
- Some people with clear RA are seronegative and never test positive for RF.
Think of RF as a suspicious footprint at the crime sceneimportant, but not enough by itself to convict RA.
Anti-CCP (Anti-Citrullinated Protein) Antibodies
Anti-CCP (also called anti-ACPA) antibodies are a more specific marker for RA. When anti-CCP is clearly positive:
- It strongly increases the likelihood of RA.
- It’s often associated with a higher risk of more aggressive joint damage over time.
You can have RA with a negative anti-CCP test (again: no single test is definitive), but a positive result is a big clue your doctor won’t ignore.
Inflammation Markers: ESR and CRP
Two common blood tests measure general inflammation:
- ESR (erythrocyte sedimentation rate), also called sed rate
- CRP (C-reactive protein)
High ESR or CRP doesn’t prove RA, but it indicates your body is in “inflammation mode.” These markers are also used later to monitor how well treatment is controlling disease activity.
Other Helpful Lab Tests
Your doctor may also order:
- Complete blood count (CBC) to look for anemia or high platelets, which may reflect chronic inflammation.
- Metabolic and liver panels to check overall health and readiness for certain medications.
- Tests for other autoimmune diseases (such as ANA for lupus) if symptoms are atypical.
These tests help rule out other causes of joint pain and prepare for safe treatment if RA is diagnosed.
Imaging: Seeing Rheumatoid Arthritis in Your Joints
Imaging studies add another dimension to RA diagnosisliterally. They show what’s happening inside your joints, not just what can be felt on the surface.
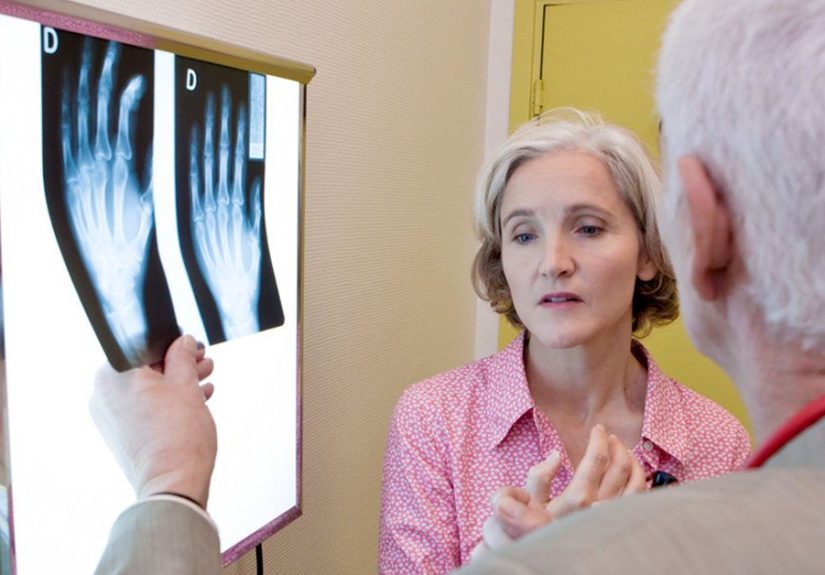
X-Rays
Standard X-rays are often the first imaging studies your doctor will order. In early RA, X-rays might look normal or show subtle changes. Over time, they can reveal:
- Narrowing of joint spaces (from cartilage loss)
- Erosions, or small “bites” out of the bone
- Misalignment or deformities in more advanced disease
Even if your X-rays look okay now, they provide a baseline for comparison years down the road.
Ultrasound and MRI
Modern RA diagnosis increasingly uses ultrasound and sometimes MRI, especially in early or unclear cases. These tests can:
- Detect subtle synovitis (inflammation of the joint lining) before X-rays show damage.
- Show power Doppler signals, indicating active blood flow associated with inflammation.
- Reveal bone marrow edema and early erosions on MRI.
You won’t always need these advanced imaging tests, but they can be especially helpful if your labs are negative or your diagnosis is uncertain.
The 2010 ACR/EULAR Classification Criteria: The Scoring System Behind RA
To bring more consistency to RA diagnosis and research, the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) developed the
2010 RA classification criteria. Rather than relying on late-stage damage, these criteria focus on early features of disease.
Who the Criteria Are For
The criteria apply to people who:
- Have at least one joint with definite clinical synovitis (clear swelling), and
- Do not have another better explanation (such as gout, osteoarthritis injury, or infection).
Once those conditions are met, the doctor uses a point-based system to classify whether RA is present.
The Four Scoring Categories
The criteria assign a total score from 0 to 10, based on four domains:
-
Joint involvement (0–5 points)
More small joints involved (like finger and toe joints) generally means a higher score.
For example, several small joints on both hands typically scores more points than a single large knee joint. -
Serology: RF and anti-CCP (0–3 points)
Negative tests score 0, low-positive RF or anti-CCP score intermediate points, and high-positive levels score the most. -
Acute-phase reactants: ESR or CRP (0–1 point)
Normal levels score 0; abnormal levels earn 1 point. -
Symptom duration (0–1 point)
Symptoms lasting less than six weeks score 0; symptoms lasting six weeks or longer score 1.
A total score of 6 or more out of 10 classifies a person as having “definite RA” under these criteria.
Classification vs. Diagnosis: Important but Subtle
One important nuance: these are classification criteria, designed mainly for research and consistency.
In real clinics, doctors use them as a helpful frameworkbut they are not the only deciding factor.
An experienced rheumatologist may diagnose RA even if you don’t hit a score of 6 yet, especially if imaging is convincing.
On the flip side, they may hesitate to label it RA if other conditions or red flags are present, even if your score is technically high.
Conditions That Can Mimic Rheumatoid Arthritis
Part of diagnosing RA is making sure it’s not something else entirely. Common mimics include:
- Osteoarthritis – more mechanical, often affects weight-bearing joints and has less prolonged morning stiffness.
- Lupus or other connective tissue diseases – may cause joint pain plus skin rashes, kidney issues, or other organ involvement.
- Psoriatic arthritis – associated with psoriasis, nail changes, and often more asymmetric joint involvement.
- Gout or pseudogout – sharp, episodic attacks, often in one joint at a time.
- Viral arthritis – can cause short-term joint pain that resolves after the infection.
- Fibromyalgia – widespread pain and fatigue, but without the inflammatory joint swelling and lab changes seen in RA.
This is where the combination of history, physical exam, lab tests, and imaging really shines. Your doctor isn’t just looking for RAthey’re trying to correctly name whatever is actually going on.
What the RA Diagnostic Journey Often Looks Like
From Primary Care to Rheumatologist
Many people start with their primary care provider, who:
- Hears your symptom story
- Orders basic labs like CBC, ESR, CRP, and sometimes RF
- Rules out obvious infections or injuries
- Refers you to a rheumatologist if inflammatory arthritis is suspected
A rheumatologist is a specialist in arthritis and autoimmune diseases. They’re the ones most experienced in applying RA criteria, interpreting borderline lab results, and choosing treatments.
Your First Rheumatology Visit
Expect a deep dive into:
- Your full symptom history (be prepared to go over months or even years).
- Detailed joint-by-joint examination.
- Review of prior tests and imaging.
- New orders for RF, anti-CCP, ESR/CRP, and sometimes additional markers or imaging.
At the end of this visit, you may receive:
- A firm diagnosis of RA
- A “probable RA” or “undifferentiated inflammatory arthritis” label
- Or a decision to monitor over time if the picture isn’t fully clear yet
Living in the “Maybe” Zone: Undifferentiated Arthritis
Not everyone meets RA criteria right away. Some people have early inflammatory arthritis that doesn’t yet fit a specific category; this is sometimes called
undifferentiated inflammatory arthritis.
In this phase, your doctor might:
- Start milder treatment while watching closely for progression.
- Repeat labs after a period of time.
- Use imaging like ultrasound to look for more convincing inflammatory changes.
It can be frustrating to live in diagnostic limbo, but it’s common. Keeping track of your symptoms, staying engaged with follow-up visits, and asking questions can make this stage more manageable.
How Often Are Tests Repeated?
After diagnosis, the goal shifts from “What is this?” to “How active is it, and is treatment working?”
Your rheumatologist may:
- Check ESR and CRP periodically to track inflammation.
- Repeat CBC and chemistry panels to monitor medication side effects.
- Order periodic X-rays or other imaging to ensure your joints aren’t quietly worsening.
Repeat testing is personalized; some people need frequent labs early on, then less often once their RA is stable.
Real-Life Experiences with Rheumatoid Arthritis Diagnosis
Statistics and scoring systems are helpful, but if you’re in the middle of this process, what you really want to know is: “Is what I’m feeling normal?”
Here are some common experiences many people share on the road to an RA diagnosis.
“I Thought I Was Just Getting Older”
A lot of people initially chalk up their joint pain to age, stress, or overuse. When your hands are stiff and puffy in the morning, it’s easy to blame your keyboard, your phone, or that one time you moved a couch by yourself.
Over time, though, patterns emerge: the stiffness lasts longer, small tasks like opening jars or turning doorknobs become harder, and normal aches just don’t explain it anymore.
For many, the turning point is when everyday taskslike brushing teeth, buttoning shirts, or walking a few blocksstart to feel like mini workout challenges.
“My Tests Were Negative, but Something Was Clearly Wrong”
One of the most confusing experiences people report is being told their blood tests are “normal” even when their joints are obviously unhappy.
This is especially common in seronegative RA, where RF and anti-CCP are negative.
It’s emotionally tough: you hurt, but you worry that normal labs mean your doctor might not believe you. The good rheumatologists know this and rely heavily on physical exam, imaging, and clinical judgmentnot just lab numbers.
If this sounds like you, it’s okay to ask directly, “Could this be seronegative RA, and how are you thinking about that possibility?”
“Getting a Name Was Scaryand Weirdly a Relief”
When the diagnosis of RA finally lands, people often describe a mix of fear and relief. Fear because “chronic autoimmune disease” is not the phrase anyone wants on their chart; relief because now, finally, there’s a name and a plan.
Many patients say the first real sense of hope comes when their rheumatologist explains modern treatment options: DMARDs, biologics, and targeted therapies that can keep joints functioning and people working, parenting, traveling, and living their lives.
Knowing that you’re not powerlessand that there’s a team and a strategycan transform the diagnosis from a life sentence into a manageable condition.
“What Helped Me Cope During the Diagnostic Process”
While everyone’s story is unique, a few practical strategies come up again and again:
- Keeping a symptom journal: Jot down which joints hurt, how long morning stiffness lasts, and what activities are hard. This helps your doctor see patterns.
- Bringing a support person: A partner, friend, or family member can help remember details and ask questions you might forget.
- Being honest about function: If pain and stiffness are messing with your job, parenting, or sleep, say so. This matters when deciding on treatment intensity.
- Asking for plain language: It’s okay to say, “Can you explain that again in simpler terms?” Medicine is full of jargon; you’re allowed to ask for translation.
Many people also find comfort in connecting with others who have RAthrough support groups, online communities, or patient organizations. Hearing how others navigated their diagnostic maze can make you feel less alone and more empowered.
“Looking Back, I Wish I’d Gone Sooner”
A very common reflection from people living with RA is: “I wish I had taken my symptoms seriously earlier.”
Waiting months or years because you’re busy, worried about overreacting, or hoping it will “just go away” can delay diagnosis and treatment.
If your joints are swollen, stiff for long periods in the morning, and painful on most daysand especially if this has gone on for more than six weeksconsider that your body might be sending you a memo you shouldn’t ignore.
The Bottom Line
Rheumatoid arthritis diagnosis is a careful process, not a quick yes-or-no blood test. Doctors combine:
- Your story and symptom pattern
- Physical exam findings
- Blood tests like RF, anti-CCP, ESR, and CRP
- Imaging such as X-rays, ultrasound, or MRI
- The 2010 ACR/EULAR classification criteria
Getting an accurate diagnosis early matters because it opens the door to treatments that can protect your joints, reduce pain, and maintain your quality of life.
If you recognize yourself in the descriptions here, talk with a healthcare provider or ask for a referral to a rheumatologist. You deserve clear answersand a plan.
And remember: this article is for information and encouragement, not a substitute for personal medical advice. Your joints, your labs, and your story are unique; the best diagnosis happens in partnership with a qualified healthcare professional.